C.L.E.A.N Tobacco Recovery™

All Addiction Is Bonding: The Neuroscience of Attachment, Tobacco, and the Path to Lasting Freedom
Guzalia Davis
There is a question worth sitting with before we talk about tobacco addiction — or any addiction. The question is this: why do we not call love an addiction?
The neurochemistry is nearly identical. A person newly in love shows elevated dopamine activity in the brain's reward circuitry, reduced activity in the prefrontal cortex — the seat of rational judgment — heightened preoccupation with the object of attachment, disrupted sleep and appetite, and measurable withdrawal symptoms when separated from the loved one. The behavioral patterns of early romantic love and early-stage substance dependence are, at the neurological level, almost indistinguishable.
We do not call love an addiction because we approve of the object. We call nicotine dependence an addiction because we do not. But the mechanism — the neurological process by which the brain forms a deep, persistent, motivationally powerful bond with something outside itself — is the same. Understanding this is not a philosophical abstraction. It is the most practically useful thing a person struggling with tobacco can learn about their own brain.
The Bonding System: What the Brain Is Actually Doing
The human brain evolved with a bonding system — a set of neurological structures and neurochemical processes whose primary evolutionary function was to ensure that we formed deep, durable attachments to the things necessary for survival and reproduction: food, safety, social connection, sexual partners, and offspring.
This system is anchored in the mesolimbic dopamine pathway — sometimes called the reward pathway — which runs from the ventral tegmental area (VTA) deep in the brainstem through the nucleus accumbens and into the prefrontal cortex. When the brain encounters something that it registers as survival-relevant, this pathway releases dopamine. Not in proportion to pleasure exactly, but in proportion to significance — to the degree to which the brain has learned that this thing matters.
Dopamine does not produce happiness. This is one of the most consequential misunderstandings in popular neuroscience. Dopamine produces wanting, seeking, and anticipatory drive. It is the neurochemical of motivation and attachment — the force that says this matters, pursue this, return to this. The pleasure that follows is produced by other systems, particularly opioid and serotonergic pathways. But it is dopamine that builds the bond. It is dopamine that makes something feel necessary.
The brain does not distinguish between bonds we approve of and bonds we don't. It bonds to whatever it has learned to associate with relief, reward, and the resolution of distress — regardless of whether that thing is genuinely good for the organism.
Oxytocin, Habit, and the Architecture of Attachment
Dopamine is not the only neurochemical involved in bonding. Oxytocin — often called the bonding hormone — plays a critical role in establishing the emotional depth and social significance of attachments. Oxytocin is released during physical touch, social connection, moments of trust and safety, and the experience of being seen and understood. It deepens the dopamine bond by adding emotional weight, creating the felt sense of connection rather than mere desire.
Over time, repeated activation of the reward pathway in the presence of a specific stimulus produces a third layer of bonding: habit formation through the basal ganglia. The basal ganglia encode sequences of behavior that have been reliably associated with reward, compressing them into automatic, low-energy routines that operate below the level of conscious decision-making. This is the neurological infrastructure of habit — and it is why behaviors that began as conscious choices become, over time, automatic responses to environmental cues.
Taken together, these three systems — dopamine-driven motivation, oxytocin-mediated emotional attachment, and basal ganglia-encoded habit — constitute the full architecture of bonding. They operate in exactly the same way whether the object of attachment is a person, a place, a piece of music, or a substance. The brain does not have separate bonding systems for approved and disapproved attachments. It has one system, and it uses it without moral discrimination.
Healthy Bonds and Addictive Bonds: The Same Mechanism, Different Objects
Consider what happens neurologically when a person falls in love with another person, develops a deep relationship with a creative practice, or forms a profound connection with a place or community. The dopamine system fires in anticipation of contact. Separation produces a deficit state — withdrawal, in the literal neurological sense — that motivates reunion. The prefrontal cortex, the brain's center of rational evaluation, is partially suppressed, reducing the person's ability to objectively assess the costs of the attachment. Over time, the basal ganglia encode the behavioral routines associated with the bond, making them automatic.
This is also, precisely, what happens with tobacco.
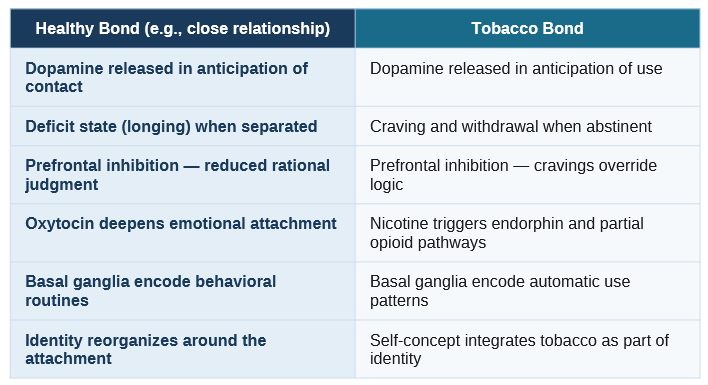
The table above is not meant to romanticize tobacco addiction. It is meant to make visible what the brain has actually done — and why the experience of addiction feels so much more like love than like a bad habit. The person who has used tobacco for twenty years is not failing to choose rationally. They are in a bond, formed by the same neurological machinery that produces every other meaningful attachment in their life. The fact that the object of that bond is harmful does not change the depth or the reality of the neurological relationship.
How Tobacco Specifically Hijacks the Bonding System
Nicotine is neurochemically extraordinary in its ability to activate the bonding system. It binds directly to nicotinic acetylcholine receptors in the VTA, triggering dopamine release in the nucleus accumbens at levels that significantly exceed what natural rewards typically produce. It does this rapidly — within seconds of inhalation or mucosal absorption — creating a tight, precise temporal association between the behavior and the reward that accelerates conditioning.
Over time, the brain adapts to the abnormally elevated dopamine stimulation by reducing its own baseline dopamine production and downregulating receptor sensitivity. The result is a neurological state in which the person no longer uses tobacco to feel good — they use it to feel normal. Without nicotine, the brain is in genuine deficit. The experience of not using tobacco is experienced as deprivation, distress, and incompleteness — not because tobacco is genuinely necessary, but because the brain has reorganized its baseline around its presence.
The Oral Bond in Smokeless Tobacco
For smokeless tobacco users, the bonding mechanism has an additional sensory layer that is not present in smoking. The prolonged physical contact of tobacco against the oral mucosa — the weight, the texture, the specific position — creates a somatic dimension of the bond. The body itself has bonded to the sensory experience. This is why oral substitution strategies are essential in smokeless tobacco cessation and why the experience of an 'empty mouth' in early recovery can feel, to the person experiencing it, disproportionately distressing. The nervous system is registering the absence of something it has come to regard as a normal part of embodied experience.
The Emotional Bond: When Tobacco Becomes a Relationship
Perhaps the most clinically significant dimension of tobacco bonding — and the most frequently overlooked in standard cessation approaches — is the emotional function. For many long-term users, tobacco has been a reliable companion through the defining experiences of their lives. It was there during stress, grief, celebration, loneliness, boredom, and fear. It never rejected them. It never let them down. It was always available, always predictable, always chemically effective.
This is not a metaphor. At the neurological level, the brain has formed a genuine attachment relationship with tobacco — one with the same emotional weight and the same separation distress as any other significant bond. Treating cessation as a simple behavioral adjustment — just stop — ignores the grief dimension that many people experience when they quit. The loss is real. The bond was real. Acknowledging this is not weakness. It is clinical accuracy.
You did not fail to quit because you lacked willpower. You failed because willpower is a conscious-brain tool, and your bond with tobacco lives in a part of the brain that operates below conscious control. You need an approach that works at the level where the bond was formed.
Replacing the Bond: The Therapeutic Pathway
Understanding addiction as bonding does not just reframe the problem — it directly points toward the solution. If the brain formed a deep bond through a specific neurological process, then recovery requires not the elimination of that process but its redirection. The bonding capacity is not pathological. The object of the bond is. The task of cessation, properly understood, is not to destroy the brain's bonding machinery — it is to give that machinery better things to bond to.
Step One: Understand What the Bond Has Been Providing
Every tobacco bond is providing something: stress relief, focus, social belonging, oral satisfaction, emotional comfort, a sense of self, a daily structure. The first step in therapeutic redirection is to map these functions with precision — not in general terms, but specifically, for this person, in these contexts. What has tobacco been doing that nothing else has been doing as reliably or as well? The answer to this question is not an indictment. It is a clinical map.
Step Two: Address the Subconscious Layer Directly
Because the tobacco bond is encoded in the subconscious — in the basal ganglia, in the emotional memory networks of the limbic system, in the somatic patterns of the body — it cannot be fully addressed through conscious behavioral change alone. Approaches that work at the subconscious level are required: clinical hypnotherapy, which bypasses the critical faculty and communicates directly with the conditioned patterns that drive automatic behavior; somatic regulation techniques that retrain the body's habitual responses; and neuro-linguistic programming methods that interrupt and replace the automatic behavioral sequences encoded over years of use.
This is the neurological rationale for hypnotherapy in tobacco cessation — not mysticism, not suggestion in the popular sense, but a clinically grounded methodology for accessing and repatterning the subconscious layer of the addiction where willpower-based approaches cannot reach.
Step Three: Build New Bonds Deliberately
The most durable recoveries are not characterized by absence — by the removal of tobacco and the effortful maintenance of a gap. They are characterized by the deliberate construction of new bonds that activate the same neurological systems tobacco was activating, through objects and practices that genuinely serve the person's health and wellbeing.
This means identifying what the person already has the capacity to bond to: physical practices, creative engagement, social connection, connection to nature, spiritual or contemplative practice, meaningful work. It means exposing the person to these things consistently and with sufficient depth that the bonding system begins to engage. Over time, the new bonds strengthen. The old bond, no longer being reinforced, weakens through the same neuroplastic processes that built it.
The brain does not unlearn bonds easily. But it is continuously capable of forming new ones. Every deep attachment a person has formed in their life — every friendship, every passion, every place that feels like home — is evidence of that capacity. Recovery from tobacco addiction is, at its most fundamental neurological level, the redirection of a bonding capacity that has never been the problem. It has always been one of the most human things about us.
C.L.E.A.N. Tobacco Recovery System™
The C.L.E.A.N. framework is built on this understanding of addiction as bonding — addressing tobacco dependence at every level where the bond was formed.
Contact: info@cleantobaccorecovery.com
© 2026 Guzalia Davis. All rights reserved.
C.L.E.A.N Tobacco Recovery™
Pennsylvania, USA
Email: info@cleantobaccorecovery.com
https://cleantobaccorecovery.com/
©2026. All rights reserved.